LeAnne Carswell didn’t want to waste money on her son’s rent, so she bought him a home.
Courtesy of LeAnne Carswell
A college mom bought a townhome for her son to save on student housing costs.
She thought paying upward of $12,000 a year for housing was a waste of money.
She expects to profit, or at least break even, when she decides to sell.
This as-told-to essay is based on conversations with LeAnne Carswell, 51, a real estate agent in South Carolina who decided to buy a home for her son to live in while studying at Clemson University instead of paying his rent. The conversation has been edited for length and clarity.
My son started at a sister school of Clemson University in his freshman year. So he did his first year at that tech school, and then Clemson took him in as a sophomore this year, but he lived on Clemson’s campus.
He was in a dorm with three roommates. I don’t remember how much room and board was, but I know it was a waste of money because we were just throwing it away. [Editor’s note: According to Clemson University, estimated housing costs for the 2025-2026 school year are $8,904.]
He came to me last fall and said, “We’ve got to start finding where I’m going to live in the fall of 2025.”
I thought that was so far away, but he said everybody’s going and looking. So all three of his roommates went and looked at a new high-rise near Clemson that’s the trendy place to go. It was between $1,000 and $1,200 a month — and he’d still have other roommates.
I said, “I’m not paying that.” So we started searching around for somewhere to buy rather than just wasting that money.
I had heard of other people owning properties while their kids were at school. I actually just got finished selling a home where the parents of a senior at Anderson University had owned it, and she had rented out three or four rooms. In that particular situation, she made a little bit of money.
I expect to at least make my money back
About 10 minutes from Clemson is a little city called Pendleton, South Carolina.
There were some new townhomes being built there. A Clemson soccer coach had gotten a new job somewhere in Texas and was leaving after having only owned the townhome for five months — she even had it all furnished. She bought it for $225,000, and we bought it from her for $227,000 in cash, fully furnished.
It has three bedrooms, two-and-a-half bathrooms, a one-car garage, and 1,523 square feet. All three bedrooms and a laundry room are upstairs.
The exterior of the townhome.
Courtesy of LeAnne Carswell.
We closed at the end of February, so it sat there for a while. School was still going on, so for a month, my son went back and forth between his place in Clemson and the townhome. And then he came home for two months, and we just left it vacant.
His friends went off and rented the trendy $1,000 to $1,200 a month unit somewhere else — even though I told him to tell them we’re buying something and to not do anything yet. But they all were scared they were going to be homeless.
Me being in real estate, I just kind of knew what was going on in the market. I thought, “We’re going to slow walk this.”
We did end up renting one room to a kid my son went to high school with who’s going to Clemson for $775 a month.
Then there’s the smaller bedroom, which we hadn’t done anything with this year. I don’t know if we would be able to rent it out this semester. Maybe in the spring that would be something that they could do, but I don’t know that I would get as much because it’s the smallest of the rooms.
I don’t know what I’m going to do with the townhome once he graduates. I’ve got a sister who’s got two boys, so maybe I’ll sell it to her, but we’ll see what happens.
I expect to profit or at least break even once I sell it. I wasn’t looking to lose $12,000 a year for the next three or four years — who knows how long it’s going to take him to get through school?
Do you have a story to share about buying property for your college-age children? Contact this reporter at jpandy@businessinsider.com.
Kelsey Birch remembers the crushing pressure, the sharp jerks, and the feeling of hands inside her abdomen. “I felt like I was being torn apart,” she said. “I couldn’t handle it.”
Birch, a then 28-year-old emergency dispatcher in Colorado, hadn’t gone into labor expecting surgery. She was healthy. Her first pregnancy had been going well, and her full-term baby was positioned face down — an ideal candidate for a vaginal birth. As her contractions grew stronger, a delivery room nurse urged Birch to get an epidural before the hospital anesthesiologist finished his shift. Birch agreed.
The American College of Obstetricians and Gynecologists recommends that a woman with an epidural in first-time labor push for up to four hours. Birch pushed for just over two before a doctor intervened. Her labor had failed to progress, her medical records noted, so, like one in three American women who give birth, Birch underwent a cesarean section.
The half-hour surgery began months of recovery. For weeks, Birch struggled to hold and breastfeed her newborn daughter. Her incision site was searingly painful; first as a fresh wound and again as it healed, scar tissue adhering to skin and muscle. Like many women who undergo a C-section, she learned to cope with intrusive memories of the surgery.
C-sections are now the most common inpatient surgery in America. Business Insider analyzed years of hospital delivery data from Florida, Mississippi, and Iowa and found that C-section rates can differ sharply between hospitals just miles apart — even when caring for similar, low-risk patients. Those gaps, experts say, point to how a hospital’s policies, culture, and financial incentives can push surgery rates higher, helping explain why the US consistently performs far more C-sections than global health authorities consider necessary.
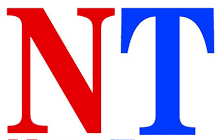
In 1970, just over 5% of babies in the US were delivered by C-section nationwide — too low to protect some women and their babies. That rate tripled within a decade. Now, for nearly 20 years, over 30% of babies in the United States have been born by C-section, around double the rate the World Health Organization says is “ideal” for maternal and infant health. US doctors perform these surgeries 60% more frequently than doctors in France, and nearly double the rate of Finland and Sweden.
Many of them, maternal health experts told Business Insider, are medically unnecessary. Federal health agencies consider women with low-risk pregnancies — those who are pregnant for the first time, are at full term, are not delivering twins, and whose babies are head-down rather than breech — the least likely group to require surgery to safely deliver their babies. Yet more than a quarter of those women delivered by C-section in the US in 2023, the most recently available year with national data.
One large study estimates that as many as 19% of all births should be C-sections to protect women and their babies, leaving as many as 13% possibly performed needlessly in the US.
That suggests roughly one in 10 pregnant American women — nearly half a million women each year — are operated on unnecessarily, undergoing major abdominal surgeries that carry a higher risk of hemorrhage, blood clots, and infection, and leave women more likely to develop dangerous complications in their future pregnancies.
It’s not because women are asking for more C-sections. Only an estimated 2.5% of US babies are born by elective C-section each year. Instead, experts say, the reason behind the high C-section rate largely comes down to the structure of the American medical system.
C-sections are more profitable, predictable, and are perceived to be more protective against lawsuits than vaginal births, according to experts and multiple studies. They say health systems looking to keep operating rooms full, revenue up, and liability risk minimized are indirectly incentivized to keep surgery rates high.
Put plainly, a high C-section rate may just be better for business.
When C-sections hurt more than they help
C-sections are often critical, sometimes lifesaving procedures.
In medical emergencies, like when the placenta completely blocks the cervix or an umbilical cord slips down past the baby, a C-section is mandatory. Failure to promptly perform the surgery can disable or kill the woman, her baby, or both. Other factors — including a pregnant woman’s age, whether she’s obese, or if she’s diagnosed with diabetes or pre-eclampsia — all increase the chance that a C-section is the safest way to deliver a baby.
To deliver a baby by C-section, a surgeon dissects through seven layers of body tissue: skin, fat, fascia, muscle, peritoneum, uterus, and amniotic sac. Doctors first use a scalpel; later, they may use their fingers or a blunt tool. Like any abdominal surgery, it also presents immediate risks, including infections, hemorrhages, blood clots, or injury to other organs.
The risks increase with additional C-sections, and a woman is far more likely to have another C-section once she’s had her first. In 2021, 86% of women who previously had a C-section underwent the surgery again to deliver their next baby. While studies show that as many as 80% of women who have undergone a prior C-section can safely deliver their next baby vaginally, many hospitals nationwide ban women who have had a C-section from attempting a later vaginal birth, citing safety and liability concerns. Each additional surgery will increase her risk of developing severe complications, like placenta accreta, which almost always requires a hysterectomy to prevent hemorrhaging.
These complications can sometimes turn deadly. While rare, the United States has the highest rate of maternal mortality among high-income countries — 18.6 deaths per 100,000 live births in 2023 — and a woman who receives a C-section is up to five times more likely to die due to pregnancy-related causes than a woman who delivers vaginally.
Even when the surgery goes as expected, some women describe the experience as extreme, even traumatic. Women are anesthetized, but most choose to remain conscious to witness the birth of their child. While some women who spoke with Business Insider said their surgeries were unremarkable and felt little of the procedure, others told Business Insider they still felt the snagging pull of the scalpel, intense pressure, and sometimes shocking pain. Their memories of the surgery are punctuated with specific detail: their arms held outstretched, pinned in restraints secured to the operating table; their bodies trembling; and their newborns held amid IV lines and the surgical drape.
Edgar Barragan Juarez/Getty Images
After a C-section, some women endure weeks or months of painful recovery, much longer than women who deliver vaginally. Women told Business Insider they struggled to breastfeed, shower, and get out of bed to care for their newborns. Some suffered painful infections along their 4- to 6-inch surgical incisions. Others weathered panic attacks, nightmares, and lingering anxiety.
The hospital you choose can affect how likely you are to get a C-section
Doctors delivering babies have to make tough calls. If a fetal heart rate monitor alerts that a baby is in distress, or if a woman’s labor is so prolonged that she or her baby is at risk of suffering severe injury, a doctor might feel compelled to intervene.
Even if the medical necessity of C-section is ambiguous, “I can’t really gamble,” said Dr. Elizabeth Langen, an OB-GYN and a clinical associate professor at the University of Michigan who studies C-section rates. Doctors may choose to perform a C-section because “it’s devastating when a baby is born and isn’t doing well,” she said. “You keep thinking, ‘Is there something else I could have done?'”
The health and safety of a woman and her baby aren’t always the only influences at play.
Controlling for a constellation of factors — hospital obstetric care levels, delivery volume, urban or rural location, maternal age, race, health, and income — multiple studies show that one of the strongest predictors of whether a woman will get a C-section is which hospital she delivers in.
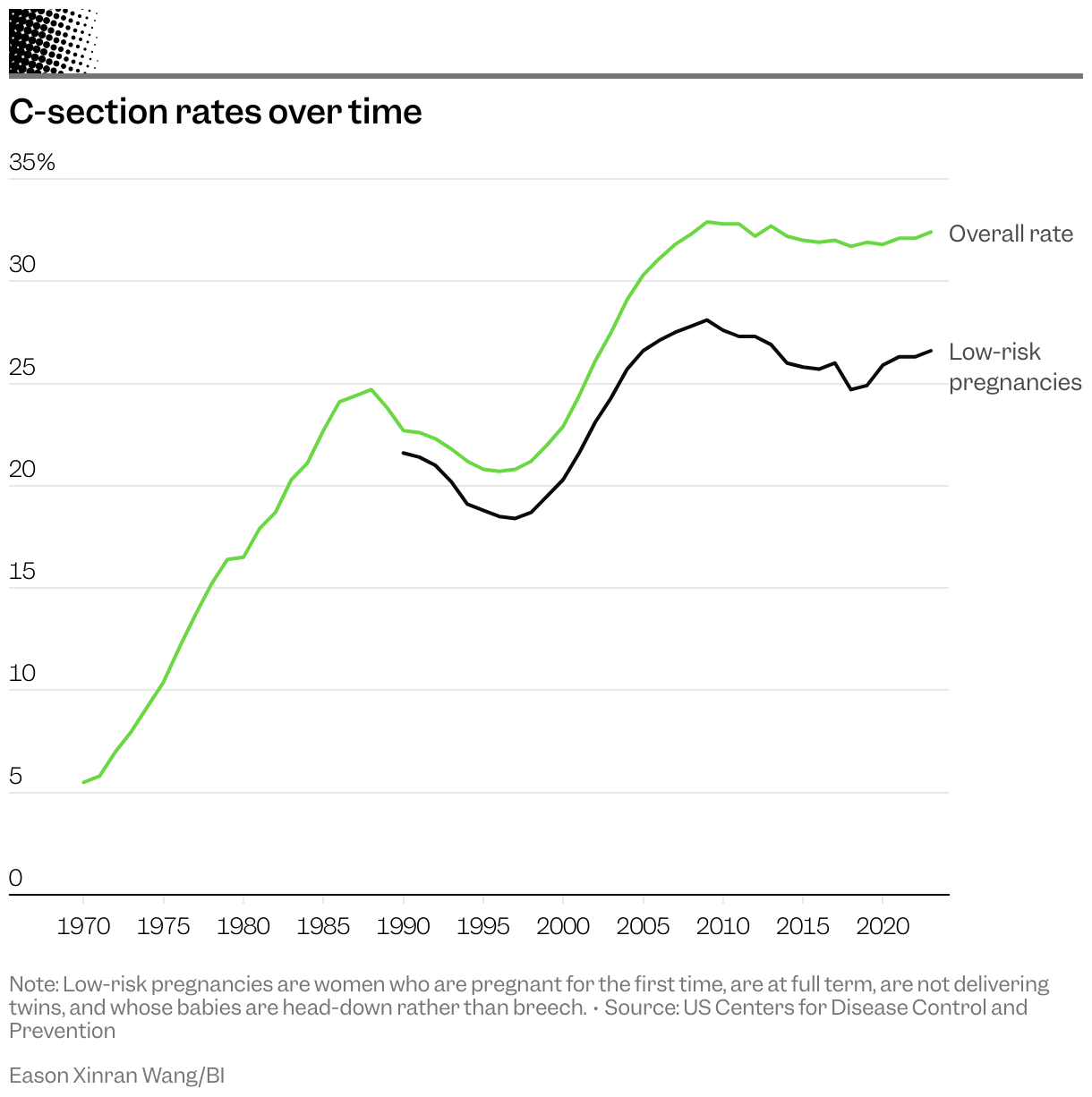
Business Insider requested data on hospital delivery data from all 50 states and DC, and analyzed data from three states that responded first to the request or had already published the data publicly: Florida, Mississippi, and Iowa. Business Insider’s analysis reveals huge variations in C-section rates from one neighboring hospital to another — suggesting a woman’s chance of undergoing a C-section is affected by her choice between two close-by hospitals.
A 15-minute drive is enough to swing outcomes. In 2019, the average rate of C-sections at one Palm Beach County hospital in Florida was 26% higher than at a hospital less than 5 miles away in a similarly majority white, wealthy area. Between 2010 and 2019, Business Insider found similar instances in Broward, Duval, Miami-Dade, and at least five other Florida counties. The hospitals all had similar levels of obstetric care and numbers of babies delivered.
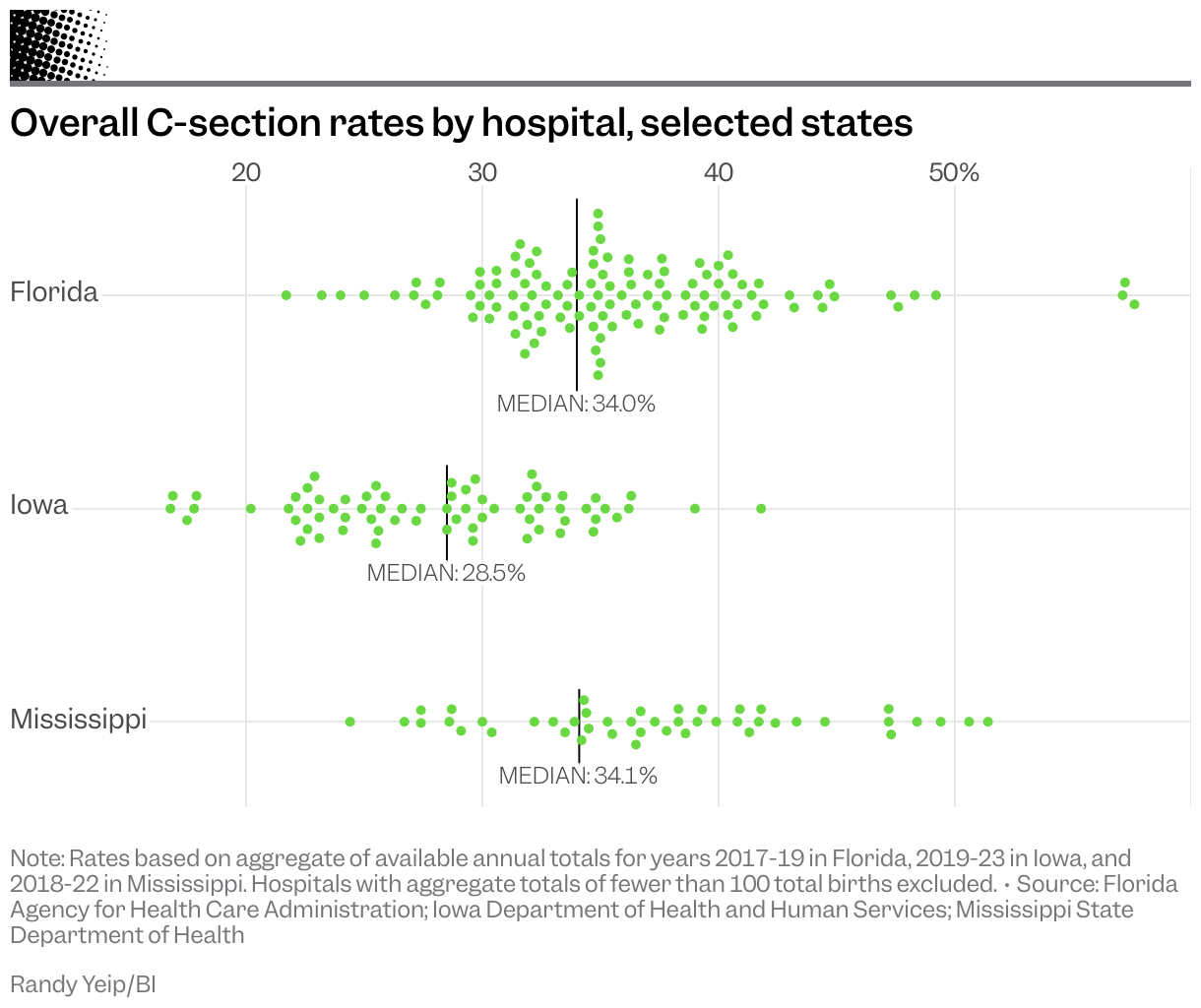
Similar patterns were found in Mississippi, where C-section rates are among the highest in the country, as well as in Iowa, where C-section rates are among the lowest nationwide. Doctors at a hospital in northwest Iowa, performed surgeries on women who were pregnant for the first time at a rate 65% higher than doctors at a comparable hospital 15 minutes away, according to Business Insider’s analysis of aggregate five-year hospital birth data from 2019 to 2023.
For C-sections performed on low-risk pregnancies, differences in hospital rates may be more telling, experts told Business Insider, as surgeries performed in this category are more likely to have been medically unnecessary.
In Mississippi, which has the highest rate of C-sections on low-risk pregnancies in the country, some hospitals had low-risk pregnancy cesarean delivery rates that swung as low as 14%. Doctors at other hospitals performed C-sections on 45% of all women with low-risk pregnancies, according to the analysis of data from 2022.
How a hospital operates — its workplace culture, administrators’ priorities, and the type and number of staff employed, particularly nurses or midwives — can dramatically impact how many cesarean deliveries its doctors perform, said Dr. Emily White VanGompel, a family medicine doctor and professor at the University of Illinois Chicago who studies how organizations impact C-section rates.
Hospital administrators and care staff can foster cultures more supportive of vaginal birth, White VanGompel said. Conversely, they can also implement policies and care standards that cause doctors to intervene more in a woman’s labor.
Some hospitals that treat women with high-risk pregnancies may require a high C-section rate to most safely deliver their patients’ babies. A risk-adverse hospital may also lead doctors to perform more medical interventions in part to minimize its risk of a lawsuit, said Louise Roth, a sociology professor at the University of Arizona who studies how organizations and medical malpractice influence maternal health, including C-section rates.
Doctors may then practice medicine in ways that evidence-based studies show can increase the chance of a C-section: induce labor more often, continuously monitor more fetal heart rates in low-risk pregnancies, and interrupt women who push for more than a few hours — all procedures that are more insulating in the case of a lawsuit, Roth said.
OB-GYNs are among the doctors most likely to face a legal threat at least once in their career, a 2023 study found, and a lawsuit filed over the serious harm or death of a baby can result in tens of millions of dollars in jury awards.
“People often will teach young obstetricians that you don’t get sued for doing a C-section, you get sued for not doing a C-section,” Langen said.
Roth said doing more also satisfies another hospital demand: billing more procedures and garnering more reimbursements.
“Intervening more almost always means a C-section,” Roth said, “But less intervention means less money.”
In Kelsey Birch’s case, the hospital where she delivered disclosed in a 2025 survey that it had an average C-section rate 22% higher than the state average.
Why the US performs so many C-sections
A C-section is major surgery. It’s also lucrative.
Providers in the 1970s and 1980s responded to “market shocks” — dips in the birthrate that undercut their profits — by performing more highly reimbursed C-sections, a pioneering 1996 study found. A 2017 study revealed that California women, meanwhile, were 12% more likely to receive a C-section if their doctor was reimbursed just $420 more for the surgery than for a vaginal delivery.
On average, US insurers in 2020 paid $17,103 for a C-section and $11,453 for vaginal birth, according to one 2022 study. Physicians were paid about 16% more, on average, for a C-section than a vaginal delivery, according to a 2015 study. Because a C-section takes much less time, it’s more cost-effective for both providers and hospitals.
While researchers in the early 2000s found that pregnant women who are older, obese, or who have other preexisting health issues undergo C-sections at higher rates, more recent studies have since found that controlling for these and many other patient factors doesn’t eliminate the wide swings in C-section rates between hospitals or explain the high C-section rate nationwide.
Research has repeatedly shown the connection between profits and surgical deliveries. Women who gave birth at for-profit hospitals were more likely to deliver by C-section; women were more likely to undergo a C-section at hospitals that reap higher profits from each C-section than hospitals where the procedure is less lucrative; and Florida obstetricians increased the number of C-sections they performed after their practices were acquired by management companies that prioritized increasing practice revenue.
Some women are more likely to get the surgery. Black women nationwide undergo C-sections at higher rates than white women. Doctors in hospitals across New Jersey, for example, were much more likely to give Black women unnecessary C-sections to fill empty operating rooms and maximize payouts.
Directly incentivizing doctors to perform more C-sections is illegal, but other incentives like bonus payments for bringing in more money to the practice or mandatory practice revenue thresholds can influence doctors to increase the number of surgeries they perform, said Ambar La Forgia, an associate professor at Haas School of Business at the University of California, Berkley, and the author of the Florida study.
“It’s a known fact that C-sections reimburse more highly than a vaginal birth, but they’re also easier to do and easier to schedule,” said La Forgia, making them attractive procedures to healthcare companies looking to boost their bottom line.
In some cases, overuse becomes criminal. In January 2025, the Department of Justice accused Chesapeake Regional Medical Center in Southeast Virginia of fraudulently billing for unnecessary procedures, including C-sections tied to the hospital’s former chief obstetrician, Javaid Perwaiz. Prosecutors said Perwaiz routinely falsified records to justify early labor inductions and C-sections timed to his weekend surgery block. The pattern was so blatant that hospital staff nicknamed the resulting NICU admissions the “Perwaiz special,” according to a federal indictment.
The indictment called the fraud “patently obvious” and an “open secret” that was documented repeatedly to hospital leadership and ignored. The hospital turned a blind eye, the indictment said, because Perwaiz’s actions reaped a financial reward.
The hospital had been aware of red flags around Perwaiz’s history for decades, the indictment charged. Following Perwaiz’s federal tax fraud conviction in 1996, another obstetrician at Chesapeake Regional warned the Virginia medical board that “unnecessary gynecologic surgery is a growth industry in Chesapeake,” according to the indictment, and that Perwaiz might be incentivized to perform even more surgeries to pay off his fraud debts.
Around the same time, the indictment charged, Chesapeake Regional’s president wrote a letter to the medical board supporting the reinstatement of Perwaiz’s medical license, citing his value to the hospital’s bottom line.
The Chesapeake, Virginia offices where Dr. Javaid Perwaiz used to work out of.
The Washington Post via Getty Images
Perwaiz was charged in a separate criminal case in 2019 and convicted in 2021 for performing medically unnecessary surgeries, including C-sections. He was sentenced to 59 years in prison. His lawyers declined to comment on Business Insider’s reporting.
Dr. Nick Oberheiden, Chesapeake Regional’s attorney, told Business Insider that the hospital denied any wrongdoing. “We are confident that the court and a jury will find, based on the facts, the law, and the evidence, that Dr. Perwaiz was the sole wrongdoer,” Oberheiden said.
The case against Chesapeake Regional is ongoing.
C-section rates can be lowered — if hospitals and states make it a priority
The C-section rate at each individual hospital isn’t an intractable problem, said White VanGompel, the family medicine doctor. Since hospital policies, administration priorities, and staff culture have so much bearing on increasing C-section rates, she told Business Insider, changing policy, priorities, and culture can also lower them.
In a 2024 study, White VanGompel and co-authors studied hospitals in California and Florida that focused on safely lowering their C-section rate and managed to reduce cesarean births by 5% for at least 18 months.
They found the most successful hospitals had strong leadership support, communication between care teams supportive of vaginal delivery, and a culture that empowered nurses to advocate for their patients without retribution. (Nationwide, hospitals with more nursing staff or that employ midwives are also associated with lower C-section rates.)
California also shows what’s possible at the state level. In 2015, the California Maternal Quality Care Collaborative launched a campaign with policy recommendations, financial incentives, and new public transparency requirements — including publicly publishing all hospitals’ annual low-risk C-section rates — aimed at lowering low-risk pregnancy C-section rates.
In 2014, California’s low-risk pregnancy C-section rate mirrored the country’s nationwide: 26%. Five years later, the rate had declined to 22.8% — a 12% drop.
States like Wisconsin, Illinois, and New Jersey have also seen success with initiatives meant to lower C-section rates.
These kinds of state policies and hospital-level interventions aren’t just niceties, only implemented when it’s convenient for providers and hospitals, White VanGompel said.
Women’s health is at stake, White VanGompel said. “This is what actually gets results.”
Back in Colorado, Kelsey Birch wrote a complaint letter to the administrator of the hospital where she gave birth. “I now have a scar on my uterus, which could affect any subsequent pregnancies and births,” she wrote. She feared her providers had rushed her first with the epidural, and then again as she attempted to give birth vaginally.
“I believe my cesarean could have been avoided.”
Have a tip? Contact Hannah Beckler via email at hbeckler@businessinsider.com or Signal at hbeckler.72. Use a personal email address and a nonwork device; here’s our guide to sharing information securely.
Arthur C. Brooks, a bestselling author and Harvard professor, structures his day with early morning workouts, writing blocks, and time with his family.
Jenny Sherman Photography
Arthur C. Brooks is a bestselling author, columnist, and Harvard Business School professor.
His own research helps him optimize his day so he can focus on writing and teaching.
After work, he spends quality time with his family, who mostly live with him or nearby.
This as-told-to essay is based on a conversation with Arthur C. Brooks, a Harvard professor, columnist at The Atlantic, and bestselling author of books such as “The Happiness Files.” This interview has been edited for length and clarity.
For about 12 years, I was a French horn player in Barcelona. At 28, I went back to school and got my bachelor’s degree through distance learning.
Then, I became a behavioral scientist. First, I got my master’s in economics. For my Ph.D., I focused on public policy analysis and human behavior, learning what makes people tick. I thought: “Where’s this stuff been my whole life?”
I was a professor at two universities before becoming the president of a think tank for just over 10 years. When I left,I saw a world that was growing unhappier, lonelier, and more polarized, and I wanted to do something about it.
I became a professor of practice at Harvard, but everything I do is teaching: my podcasts, my column, my books. I’m just a college professor, but I’m using these means to reach millions and millions.
Given that I have to do a lot in a day, I stack everything so my brain chemistry is optimized for work.
I wake up at 4:30 a.m. to work out
Brooks does an hour of resistance training and zone 2 cardio every day.
Jake Rosenberg
I have two objectives every morning. No. 1 is creativity and focus, because I write every day. No. 2 is managing negative affect, or mood. Like a quarter of the population, I’m above average in both positive and negative affect.
I get up at 4:30 am. There’s a lot of research that shows creativity and productivity are heightened if you get up before dawn. It’s also neurocognitively good for you to see the sunrise.
I take a multivitamin,electrolytes, and creatine before getting to the gym at 4:45 a.m. I work out hard for an hour every day, and I don’t work while working out. I’m not listening to neuroscience podcasts because I’ll be depleting dopamine, a neuromodulator of focus.
Brooks with his wife, Ester Munt-Brooks. They attend Catholic mass together whenever he’s at home.
Arthur C. Brooks
I attend Catholic mass every day at 6:30 a.m.
When I’m at home, I go with my wife, Ester. If I’m on the road, I have an app on my phone that tells me where the closest mass is. The great thing about being Catholic is that it’s like Starbucks—it’s like a franchise system, with the same product in every place.
I’m an authentically religious person, but mass is also important to me as a scientist, because I know that meditative focus is good for managing negative affect down and managing creativity and focus up.
I eat a protein bomb for breakfast
Around 7:30 a.m., I eat a protein bomb that’s high in tryptophan, an essential amino acid that helps with muscle growth. I have Greek yogurt, protein powder, nuts, and berries. This gives me around 60 grams of protein.
Then I’m good to go. From 8 a.m. to noon, I’ve got the best concentration.
I write for 3 to 4 hours
Brooks spends 3 to 4 hours a day writing.
Jenny Sherman Photography
When I’m writing, nobody gets in. I don’t take calls or look at social media.
About two and a half of my work windows are dedicated to “How to Build a Life,” the Atlantic column. I’m always 10 weeks ahead of publication, because I’m often a guinea pig for the techniques I’m writing about. If something doesn’t work, I don’t publish a column.
I also work on books, which are harder. I don’t usually throw away five paragraphs unless I’m trashing the whole column, but writing a book, I’ll write five paragraphs and say, “This is garbage, this is a dog’s breakfast.” Books can bring out just the absolute depths of despair.
I teach the rest of the day
Brooks teaches in-person classes and covers similar material in his podcasts and press interviews.
Harvard Kennedy School
Around noon, I eat another bolus of protein, usually something with cottage cheese or a salad with salmon.
For the rest of the day, I focus on teaching, whether I’m instructing courses or recording podcast episodes. This requires less dopamine than writing since I’m being asked questions instead of coming up with big ideas.
I teach leadership and happiness science classes at Harvard Business School and Harvard Kennedy School. The key to not burning out is making sure that you still have a life; I work with a lot of people who keep me organized, so I don’t have to work 12 hours a day over the weekend.
I spend time in my multigenerational household
Brooks and his wife share a house with their oldest son’s family.
Arthur C. Brooks
I’m on the road 48 weeks a year, but I’m almost always home on the weekends.
I have homes in Boston, where I teach, and northern Virginia, where my family is. When I’m in Virginia, I finish work at 6 p.m. and spend the rest of the evening with my family.
We have a multigenerational household. We asked our three kids where they wanted to raise their families so that we could help. They chose to be near the DC area, where they were also raised. It’s hard for me to commute to my job in Boston, but it’s a lot worse to commute to your grandkids.
My oldest son, 27, lives on the first floor of our house with his wife and son. Our 25-year-old son is expecting his second child; his family lives up the street. And our 22-year-old daughter is in the Marine Corps, 45 minutes away.
This arrangement is great for everybody. We eat supper as a family. I do a lot of the cooking and usually make some lean protein and vegetables. Then we all go do our own thing.
I go on 40-minute walks with my wife
The Brooks take long walks together after dinner.
Arthur C. Brooks
I’m super in love with my wife. We’ve been married for 34 years.
We always go for a 40-minute walk after dinner because it’s a good way to metabolize calories. My wife works in Catholic theology for Spanish-speaking audiences. We talk about something she read or something that I’m working on. For us, it’s go deep or go home.
We end the day by praying the rosary together, which is an ancient Catholic meditation.
I wind down without screens
My wife and I go to bed around 9 p.m., and we try not to look at screens.
I can’t afford not to be structured. I have terrible longevity in my family. I’m 61 years old; at my age, my mom had severe severe dementia, and I’m not much younger than when my dad died at 66. I don’t smoke, drink alcohol, or do any euphoric substances because they’re neurotoxic.
It’s a joy to focus on the things that I love, which are my family, my faith, and my work that lifts people up. The least I can do is design my life so I’m good at it.
Jack and Ardith Weber are a married couple who are both still working into their 80s.
Jack works at a library, while Ardith works as a senior medical patrol worker and an assistant.
Both work out of financial necessity, but said they feel fulfilled by their work.
This as-told-to essay is based on conversations with Jack and Ardith Weber, a married couple of 65 years who both still work for financial reasons. Jack, 88, works at his county’s library in Kentucky, while Ardith, 83, works as a senior medical patrol worker and an assistant for an anti-poverty organization.
Both took part in digital skills training through Goodwill, which administers the Senior Community Service Employment Program (SCSEP), a program created in 1965 to assist low-income adults 55 and older in finding work. Over $300 million in national funding to SCSEP was paused in July. Many employees in the program may lose their jobs, and many looking for work may lose access to one of the nation’s only job training programs for older Americans.
A Department of Labor spokesperson told Business Insider: “The funding for SCSEP national grantees is under review.”
The following has been edited for length and clarity.
Jack Weber: I’m 88 and work two hours every other day at our county library.
Ardith Weber: I’m 83 years old and work a maximum of 26 hours a week at two part-time jobs.
We really need to work because in 2017, we purchased a home and didn’t expect the expenses that came up, like the cost of redoing the floors.
Without my SCSEP training, I couldn’t do these jobs. It’s been such a blessing to me. The program is so considerate of elderly people. I never had to worry about being mistreated and have been shown respect and dignity. Our memories aren’t as good as they used to be, and many times, we try to articulate what we want to say, but it doesn’t work. Taking the classes and working through situations in lessons was really helpful.
Now the government’s doing cuts and all kinds of things with grants.
We worked many different jobs across our careers
Jack: Early in my career, I did a multitude of different jobs to stay afloat. One of the most fascinating jobs I’ve ever had was my first — running a printing press.
I worked in a greenhouse and in the fields in Washington state, and was a truck driver in Seattle, working behind a street sweeper on the freeway.
Ardith: My first job was in an office doing invoices until the company moved. From there, I worked in a nursing home. After we married, I worked in adult foster care while Jack decided to go to college.
Jack: I got my bachelor’s degree in counseling and theology.
Ardith: I became a cook in the college kitchen. After Jack graduated, we went into ministry and worked at a campground. I did the support tasks like answering the telephones, teaching some classes, and scrubbing the floors.
Looking for jobs in our 60s and beyond
Jack: In 2000, I started in an SCSEP program in Cadillac, Michigan, when I was searching for a job in my 60s. I didn’t know anything about computers and wanted to learn. The program would teach me those skills, although the work I’d do wouldn’t be on a computer.
Through SCSEP, I started at the Forest Service and worked in a garage, cleaning up cars and trucks. I wanted to move to Kentucky, so I called all the different Forest Service locations to see if there were any openings. They kept telling me no. Eventually, I found an opening for the Land Between the Lakes National Recreation Area.
From there, I landed a job as a dispatcher. I did that for almost three years, and then drove a school bus for eight and a half years.
Ardith: I started at SCSEP a year after Jack and also worked at the Forest Service. I stayed at home for a while after that, then worked at a hearing aid store.
New jobs 80 years into life
Jack: In 2019, I got involved with SCSEP again, through Goodwill. I first worked for an organization called The Good Samaritan, which handed out food for low-income folks, and then I was moved to a new job with the Logan County Public Library.
Jack Weber works a few hours a week at his country’s public library.
Goodwill Industries of Kentucky
One day, I was sitting there doing the skills-building work that Goodwill requires, like learning how to use the computer. Along came the library director, who said to me, “You want to do that kind of work, Jack?” I said sure — I figured it would be a whole lot better than dusting book covers.
He took me into this back room with all these old books, and told me he wanted me to make some indexes for them. Every day, I set up my computer and sit down with a book, going through each page and looking for names. For every name I find, I write down where I found it.
Ardith: When we moved to our current home in Kentucky, we didn’t know anybody in the area, and I suspected my mental health wouldn’t be good if I stayed home, so I re-enrolled in SCSEP in 2020.
Through the program, I got jobs at a community center and a senior center. I also took basic computer lessons.
In my work now with the Kentucky Senior Medical Patrol, I give talks at senior centers and health fairs about Medicare and Medicare fraud, including how to protect yourself and what not to do.
Our jobs allow us to help people
Jack: Most people would say my job is the most boring thing you could ever do. But it gets me out of the house, and I get a lot of joy from it. There are people who come in asking if there’s anything on the shelves that would help them know what their relative looked like when they were young. They’ll sit on the floor and go through our school yearbooks. All of a sudden, I hear them say, “That’s what they looked like when they were 18. They sure don’t look like that now.”
Ardith Weber holds two part-time jobs.
Goodwill Industries of Kentucky
Ardith: My second job is as a support staff member with the Low Income Home Energy Assistance Program and Community Services Block Grant, which helps qualifying residents pay their utility bills. My supervisor does all of the interviews, and I do the filings with people’s addresses and phone numbers.
We have lots of young people who need help coming through our office — younger families who haven’t been able to find work or have disabilities. Things have gotten really expensive, and their income isn’t high enough to take care of everything.
We don’t have plans to stop working
Jack: I work two hours every other day. I used to work four hours a day, but I had a heart issue and had to lay off work.
After being home for three months, I called the director and said, “Can I please come back? I can’t stand this anymore. Sitting at home drives me nuts.” He told me that once I got clearance from my doctor, I could walk right in. I got cleared by my primary doctor; I do have to go back to my heart doctor, though.
Now, I’m thankful to be back. I told my director that I’ll work two hours every other day until I’m back up to speed.
He says he’s glad to see me and that he’s got so much for me to do. “You’ll have to be 100 years old before you can ever retire,” he says. It’s a plus for me because I don’t ever have to worry about running out of work to do.
Ardith: He tells me all about how the other ladies who work there have done this and that for him. When his computer didn’t work and he couldn’t figure it out, this gal came and helped him. I get all of that feedback when he gets home.
I hope to keep working all the time. Otherwise, I’d just sit at home with the television, which is as boring as can be. I love to garden, but physically, I just can’t do that anymore. I couldn’t ask for a better current work situation. My supervisors are encouraging and supportive.
I need to be around people; if I’m not, it does things to my mental health. I don’t want that to happen.
As #BushTok sweeps the Internet, Newsweek spoke to experts about what America’s youngest adult generation’s fondness for the president means for politics today.
Jackie Flores’s Airbnb in Clark County, with six rooms, outdoor seating, a gaming room, and a backyard pool.
Jackie Flores
Jackie Flores pays her mortgage on her six-bedroom house by being an Airbnb host.
Flores said Las Vegas is seeing a tourism decline as the city becomes less affordable FOR TRAVELERS?.
Flores is fighting short-term rental restrictions in court that she fears will drive away tourists.
Jackie Flores is an Airbnb host in Las Vegas and the founder of the Greater Las Vegas Short-Term Rental Association. She is one of a group of property owners in Clark County, Nevada, who have filed a federal lawsuit to challenge the county and state’s ability to enforce restrictions on providing short-term rentals to visitors. Airbnb has joined the lawsuit.
Clark County’s short-term rental ordinance and Nevada Assembly Bill 363 created a 2,500-foot no short-term rental buffer zone for resort hotels, a lottery-based permit system that requires hosts to register as business owners, and caps on the number of permits allowed. Clark County has primarily cited a loss of tax revenue from unreported rentals as a reason to impose restrictions.
Being an Airbnb host in Las Vegas has helped me afford a house and make ends meet during some of my most challenging times.
I now make enough through renting out rooms to cover my mortgage and other bills related to my house.
And when tourism dollars are spread around the community instead of being concentrated in a few resorts, travelers are able to enjoy a more affordable and authentic Las Vegas experience.
Now, more than 15 years into being a host in Las Vegas, I am fighting a tourism downturn and local regulations that could ban me from renting out my rooms.
Airbnb helped me become a homeowner
It was 2008, and my business had to shut down during the real estate crash, and I needed another way to make ends meet. It also just so happens that my roommate decided to move to another state, leaving the entire three-bedroom apartment to me.
At first, I worried about having strangers in my home. But guests were respectful, and what started as a short-term fix became so much more.
Before, I always feared losing my job or having another life emergency, but knowing that this is an extra income stream gave me the confidence to finally buy a house, knowing that renting out rooms could cover my mortgage.
I got to put down roots in Las Vegas and furnished the home with the money I have saved by hosting at my previous place. The house was transformed from being completely empty with nothing in the yard, to a place where people loved to stay.
Now, my six-bedroom house is just 10 to 15 minutes south of the Strip in Clark County, where most residents in the area live. It has a pool in the yard, barbecue space, outdoor seating, and a game room for travelers to enjoy when they want more space and comfort than they would get in a hotel room.
Las Vegas is battling rising costs
Over the years, Las Vegas has gotten more expensive, especially for visitors. Even locals avoid the Strip now because of how high the prices have gotten.
I recently celebrated my birthday at a resort with some friends, and for just two nights, we spent about $1,200 on a single hotel room. Drinks were $20 each at the lounge, and meals were equally pricey.
That’s why so many travelers are looking for alternatives. At my house, a group can stay for $500 a night, which is around $1,000 for a weekend. That’s for an entire home, not just one room. If guests want just a couple of rooms, the price drops even more. For families or groups, it’s a much better deal.
To fight the tourism decline, I have been working to collaborate with small businesses in my neighborhood.
Guests who stay at my place don’t just spend money with me — they go to local restaurants, markets, and shops. I’m partnering with these businesses to create incentives, like discounts and special offers, so travelers feel like they’re getting more value out of their stay.
I’m fighting short-term rental restrictions
When visitors come, it boosts everyone, not just me.
That’s why I’m currently fighting Clark County’s short-term rental restrictions that would remove our Airbnb listings if we don’t go through a complicated process to obtain a special license.
By renovating and cleaning my place to ensure that guests are able to relax, I’m also creating jobs for local cleaners, contractors, and people transporting the guests.
I’m now going through hearings for an injunctive order to block the short-term rental restrictions, but I’m trying not to let the lawsuit be my only focus. For me, it’s also about finding ways to keep tourism alive in Las Vegas. I keep my prices reasonable, I work with other small businesses, and I make sure guests feel welcome in a city that has become less affordable for so many.
Clark County told Business Insider in a statement that it cannot comment on an ongoing litigation at the moment.